MEDICINE CASE DISCUSSION
Case of a 70 year old male with ACUTE MCA territory STROKE
May 23,2021
This is online E log book to discuss our patient’s de-identified health data shared after taking his/her/guardian’s signed informed consent. Here we discuss our individual patient’s problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problems with collective current best evidence based inputs. This e-log book also reflects my patient centered online learning portfolio and your valuable inputs on comment box is welcome .
I’ve been given this case to solve in an attempt to understand the topic of “patient
clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations, and come up with diagnosis and treatment plan.
CASE DISCUSSION
- Right sided weakness of both upper and lower limb since 6 hours.
- Loss of speech since 6 hours.
- Deviation of mouth towards left
History of presenting illness:
Patient was apparently asymptomatic 6 hours ago then he developed right side upper and lower limb weakness which was sudden in onset there were no aggravating or relieving factor,It was associated with deviation of mouth to left and loss of speech
Patient took a whole bottle of toddy yesterday(22.05.2021)night without having dinner
Past history
There were no similar complains in the past
History of trauma 15 years ago following which he developed sudden onset loss of vision and spontaneously gained vision after 2 weeks
Not a known case of hypertension,diabetes mellitus,bronchial asthma,TB
Treatment history :insignificant
Surgical history : insignificant
Family history : insignificant
Personal history:
Diet:mixed
Appetite:normal
Bowel and bladder:normal
Micturation:normal
Addictions: 1 bottle of toddy per day since 40yrs and smokes 8 bidis per day since 40 years
Physical examination
Patient was examined in a well lit room, after taking informed consent.
He was conscious,aphasic, not oriented to place and time,Malnourished, thin built,Looks dehydrated
No Pallor
No Icterus
No Cyanosis:
Clubbing of fingers present
No koilonychia
No Lymphadenopathy
No Pedal oedema
No generalised edema

Vitals
BP:140/80 mmhg( before SBP was 170 mmhg)
PR: 127 bpm
Respiratory rate: 23
Temperature:98.r
GRBS:161 mg/dL
SPO2 at room air:96% on RA
Systemic examination
CVS: S1 and S2 heart sounds heard.No murmurs
Respiratory system: Bilateral air enters is present, vesicular breath sounds,dyspnoic,bilateral infraclavicular crepitations wheezes present

Per abdomen:soft, no tenderness,no hepatomegaly or splenomegaly
CNS
Conscious
Speech: no response
No signs of meningeal irritation
Motor system examination:
Tone
Right Left
a) Upper limb Decreased Increased
b) lower limb Decreased Normal
Power:
a)upper limb 1/5 4/5
b)lower limb 1/5 4/5
Glasgow scale: E4 V1 M6. (11/15)
Reflexes:
Biceps Triceps Supinator Knee Ankle
Right 3+ 3+ 2+ 3+ 2+
Left 3+ 3+ 3+ 3+ 2+
Gait:
BUCKLING GAIT(due to initial neuronal shock stage the limbs are flaccid although it is an UML lesion later it changes to a typical UMN lesion gait)
Cerebral signs:
Finger -nose coordination and
Knee-heel coordination could not be assessed as the patient didn’t obey the commands
Siriraj stroke score:
Level of consciousness- drowsy- 1
Vomiting: No- 0
Headache: yes- 1
Atheroma markers- 1*3
DBP- 80 mmhg
Constant -12
Total:-2.5( favour ischemic stroke)
Calculation:(2.5*1)+(2*0)+(2*1)+(0.1*80)-(3*1)-12= -2.5
 |
| Siriraj stroke score |
Investigations:
CBP

RFT











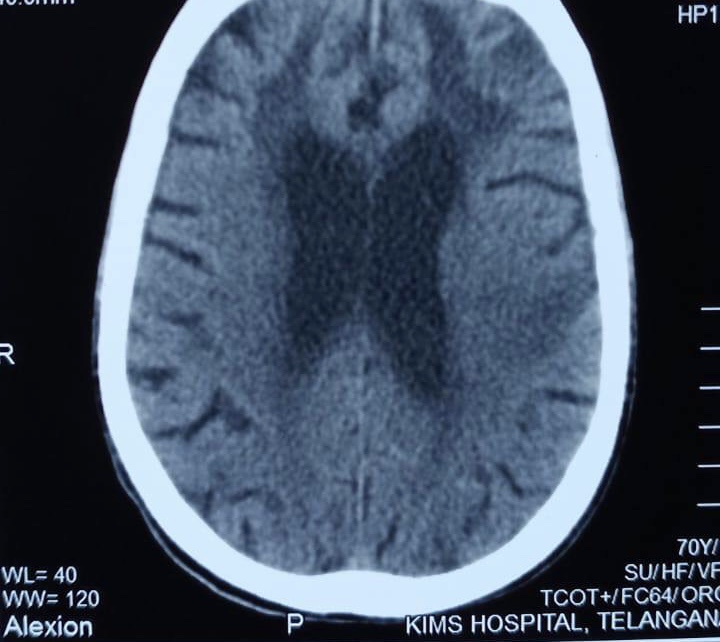


 |
| Dense MCA sign |

Provisional diagnosis:
Right hemiparesis secondary to acute MCA territory stroke
Treatment
1)Inj. THIAMINE 1amp in 100ml NS/iv/OD
2)inj. OPTINEURON 1amp in 100ml/NS/iv/OD
3)IVF-10 NS @UD +100ml/hr
4)Foley catheterisation
5)Ryles feed 100ml milk @2nd hourly
6)Tab. ECOSPRIN-AV 75/20 mg po hs
7)Bp/pr/spo2 monitoring
Comments
Post a Comment